About this information
This information is for you if you have been offered hysteroscopy as an outpatient. It may also be helpful if you are a partner, relative or friend of someone who has been offered this procedure.
Within this leaflet we may use the terms ‘woman’ and ‘women’. However, we know that it is not only people who identify as women who may need to access this leaflet. Your care should be appropriate, inclusive and sensitive to your needs whatever your gender identity.
A glossary of medical terms is available on the RCOG website at: https://www.rcog.org.uk/for-the-public/a-z-of-medical-terms/
Key points
- Outpatient hysteroscopy (OPH) is a procedure carried out in the outpatient clinic that involves looking inside your uterus (womb) with a thin telescope. Often a biopsy is also taken from the lining of the uterus (endometrium).
- You may be referred for OPH to investigate and/or treat abnormal bleeding, to remove a polyp seen on a scan or to remove a coil with missing threads.
- You can choose to have your hysteroscopy with an anaesthetic (general or regional anaesthetic), or with sedation. This is done in an operating theatre, usually as a daycase procedure.
- An OPH procedure usually takes 5-10 minutes. It can take longer if you are having any additional procedures.
- You are likely to feel some pain during and after your hysteroscopy. For the majority of women this is not severe. If a biopsy is taken, this can cause more pain. It is recommended that you take pain relief around 1 hour before your appointment.
- You do not have to continue with the procedure if it is too painful. Your hysteroscopy can be stopped at any time. Tell your healthcare professional if you want the procedure to be stopped for any reason.
- Possible risks with OPH include severe pain, feeling faint or sick, bleeding, infection and rarely damage to the wall of the uterus (uterine perforation). Sometimes it is not possible to complete the procedure in an outpatient clinic.
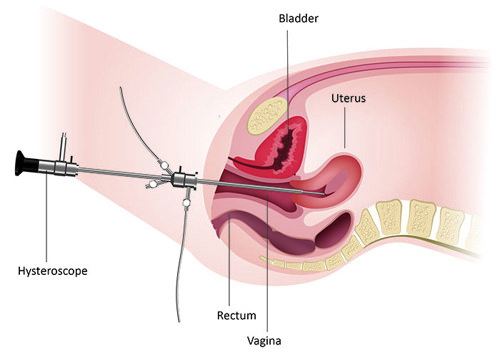
An OPH is a procedure that involves a healthcare professional looking inside of your uterus (womb), to check the inner lining and shape of your womb. This is done by passing a thin telescope-like device, called a hysteroscope, through your cervix.
[Image] A hysteroscope being used to examine the cervix:
[Image] A polyp inside the uterus which may be removed during hysteroscopy:
![[Image] A polyp inside the uterus which may be removed during hysteroscopy:](/media/i42j1fo5/outpatient-hysteroscopy-02.jpg?width=500&height=428.7090558766859)
It may be possible for an additional procedure to be done during the same visit, such as:
- Endometrial biopsy – taking a sample from the lining of the uterus. This can be done through the hysteroscope or after inserting a speculum and passing a thin tube through your cervix.
- Polyp removal – a polyp inside the uterus is a skin tag that looks like a small grape, sometimes on a stalk. Polyps are caused by an overgrowth of the lining of the uterus.
- Small fibroid removal – fibroids are knots in the muscle of the uterus that are non-cancerous. They can sometimes bulge like a polyp into the lining of your uterus and your healthcare professional may advise removal to help with your symptoms.
- Endometrial ablation – a treatment which thins or removes the lining of the uterus to treat heavy menstrual bleeding.
- Insertion of an intrauterine device - this may be a hormonal coil (IUS), such as a Mirena® or a copper coil (IUD).
- Removal of an IUD or IUS from your uterus if the threads are not visible.
You may have been referred for OPH for one of the following reasons:
- bleeding after the menopause (postmenopausal bleeding)
- to investigate something seen inside the uterus (womb) on an ultrasound scan, such as an endometrial polyp or fibroid
- heavy or prolonged periods
- bleeding between your periods
- irregular bleeding while on hormonal treatment
- removal of your coil when the threads are not visible at the cervix
- fertility concerns
- following a miscarriage
The purpose of your appointment is to find the cause of your problem and plan or undertake treatment if needed.
You must not have a hysteroscopy if there is any chance that you are pregnant. To avoid this, it is important to use contraception or avoid sex between your last period and your appointment. You may be offered a urine pregnancy test on arrival at your appointment.
It is best to keep the appointment although sometimes it can be difficult to do the procedure if there is too much bleeding. If you have any concerns, please discuss this with your healthcare professional.
Before your appointment
You should be given written information before attending your OPH appointment about what the procedure involves. This information should include contact details so you can speak to someone if you have any questions or concerns before your appointment.
You should eat and drink normally. You do not need to fast before your appointment.
You will be advised to take pain relief 1 hour before your appointment, such as ibuprofen and/or paracetamol or other pain relief medication which is effective for you.
Bring a list of any medications that you are taking with you.
You may wish to bring a friend or family member with you.
On arrival
You will meet your healthcare professional who will discuss the procedure in detail with you. If you feel anxious about the procedure, you should talk to your healthcare professional.
This will include:
- why you are being offered OPH
- any additional treatments you may be offered at the same time and;
- the possible risks, benefits and alternatives to the procedure.
They will ask for your written consent to go ahead with the OPH and you can ask any questions you may have. You can agree how to let your healthcare professional know if you want your procedure to be stopped.
If you are unsure about whether to go ahead with the procedure, your appointment can be rescheduled to allow you to have more time to make a decision that is right for you.
There will be two or three healthcare professionals in the room, including a nurse who will support you throughout the procedure. You will be given access to a private changing area. The team will then help you to get positioned in a special chair and will keep you as covered as much as possible.
You can choose to have your friend or family member with you in the room throughout the procedure if you wish.
The procedure
A hysteroscope is passed through your cervix to give a clear view of the inside of your uterus (womb). No cuts are needed. Fluid (sterile saline solution) is used to help see the inner lining of your uterus and you will feel wet as the fluid trickles back out.
If no problems are found, the actual procedure will only take about 5–10 minutes.
Sometimes, your healthcare professional may take a small sample (biopsy) from the lining of your uterus and send it to the laboratory for examination. You may feel more pain at this point and afterwards.
If a fibroid or polyp is found, your healthcare professional may offer to remove it at the same time, if you agree. Otherwise, your healthcare professional can schedule another appointment to do this. This could be as an outpatient procedure or
in an operating theatre with an anaesthetic (general or regional anaesthetic) or sedation.
During the OPH, your healthcare professional will look inside your uterus on a screen and you can also watch the screen if you choose to. Photographs of the inside of your uterus are taken and kept in your healthcare notes.
How long does the visit take?
The actual procedure may only take 5–10 minutes; however, the total visit may take up to 2 hours including consultation, having the procedure and recovery. If polyps or small fibroids are removed at the same time, the procedure may take a bit longer.
After the procedure you can stay in the outpatient clinic’s rest area for as long as you need and you will be offered pain relief if you need it.
Before you go home, you should be given information about what to expect after your OPH, including contact numbers in case you have any questions or concerns.
How will I feel afterwards?
Most women feel able to go back to their normal activities on the same day.
You may get some cramping or lower abdominal pain for several hours after the procedure, but sometimes this can last for a few days. You may also have some spotting or fresh (bright red) bleeding that may last up to 1 week.
You can shower as normal. You should avoid putting anything inside your vagina, for example, using tampons, and having penetrative sex while you are still bleeding.
You can go back to normal physical activities (including sex) when any bleeding and pain has settled.
If needed, you can take pain relief such as ibuprofen and/or paracetamol every 4 hours, or other pain relief medication which is effective for you.
If your pain is not controlled with the above medication, you should contact your healthcare professional or nearest emergency department.
What happens next?
If no problems are found, you may not need any follow-up appointments. If a biopsy has been taken, you will be contacted with the results when they become available. Your healthcare professional will discuss any further treatment with you.
- Pain during or after OPH is common. While most women experience some pain, others find it more intense. Pain relief medications can help.
- Feeling or being sick or fainting can affect a small number of women. However, these symptoms usually settle quickly. Let your healthcare professional know if you are feeling unwell during or straight after the procedure.
- Bleeding is usually very mild and is lighter than a period, stopping within a few days to a week. It is recommended that you use sanitary towels, not tampons while you are bleeding. If the bleeding does not settle and gets worse, contact your healthcare professional or nearest emergency department.
- Infection is uncommon (less than 3 in 100 women). It may appear as a smelly vaginal discharge, fever or severe pain in your abdomen. If you develop any of these symptoms, contact your healthcare professional urgently.
- Unsuccessful OPH means it has not been possible to pass the hysteroscope into your uterus (womb). Usually this happens when the cervix is tightly ‘closed’ or scarred. If this happens, your healthcare professional will discuss alternative options with you.
- Damage to the wall of the uterus (uterine perforation) – This is when a small hole is made in the wall of the uterus (womb). Rarely, this could cause damage to nearby organs. This happens in less than 1 in 200 diagnostic hysteroscopy procedures, but is slightly more common if you are having a polyp or fibroid removed at the same time. It may mean that you have to stay in hospital overnight. Usually, no more treatment is needed, but sometimes you may need a further operation to repair the hole, or damage to nearby organs.
Most women will experience some pain, and for some women it can be severe. A UK survey of over 5000 women having a hysteroscopy asked them to rate their pain out of 10, where 0 is no pain and 10 is the worst pain. One-third of women found their pain to be above 7 out of 10.
You do not have to continue with the procedure if it is too painful for you. The procedure can be stopped straight away if you are in too much pain. The nurse is there to speak on your behalf if needed and you can agree before starting the procedure on how to let your healthcare professional know if you want your procedure to be stopped.
OPH is often done without inserting a speculum, and using a thin telescope, as this is more comfortable for you. This is called vaginoscopic OPH.
If you are also having another procedure (such as polyp or fibroid removal), you might feel more pain. This will only be done with your consent.
Pain relief medications taken before your procedure helps. Your healthcare professional may offer a local anaesthetic injection into your cervix. This is usually offered when the cervix needs to be stretched to allow the hysteroscope to pass, and local anaesthetic may reduce the pain that this can cause. To give this they will need to use a speculum to see your cervix. You may be sometimes be offered an injection of local anaesthetic to the uterus (womb). The local anaesthetic injection itself can be painful but it takes effect very quickly.
Some hospitals may offer pain relief that you breathe, such as Entonox (nitrous oxide) or Penthrox (methoxyflurane), to help with your pain. If you use this, you may be advised to wait a bit longer in the hospital to recover before you can drive. You may wish to use other ways to manage pain, depending on the situation, such as a heat pack, music and other distraction techniques.
There may be other things to consider when deciding whether OPH is the right choice for you, such as:
- if you faint during your periods because of pain
- if you have experienced severe pain during a previous vaginal examination
- if you have experienced difficult or painful cervical smears
- if you have had any previous traumatic experience that might make the procedure difficult for you
- if you do not wish to have this examination when awake.
If you do not think that OPH is right for you, you can choose to have your hysteroscopy with an anaesthetic (general or regional anaesthetic), or sedation. This will be done in an operating theatre, usually as a daycase procedure.
You may still feel some pain after the procedure even when it is done with an anaesthetic, and the risks and complications are slightly higher than the outpatient procedure. If you prefer the option of having an anaesthetic or sedation discuss this with your healthcare professional who will support your choice.
You can choose not to have a hysteroscopy at all, though this may make it more difficult for your healthcare professional to find the cause of your symptoms and to offer the right treatment for you. They may then recommend a scan and a biopsy to find out more information and/or may ask you to come back if your symptoms continue.
The nature of gynaecological and obstetric care means that physical examinations are often necessary. This may involve an examination of your abdomen or an internal examination of your vagina.
We understand that for some women, including those who have experienced trauma, physical or sexual abuse, such examinations can be very difficult. Your healthcare professionals are there to provide kind and personalised care to you. If you choose not to be examined, they can discuss alternative options with you.
After explaining to you about the physical examination you are being offered, your healthcare professional will seek your consent. You should always be offered a chaperone. You could also ask for your partner, family member or friend to be in the room to support you, if you wish.
If you feel uncomfortable, anxious, distressed or in pain at any time before, during, or after an examination, please let your healthcare professionals know, as they are there to support you.
If you find this difficult to talk about, you may communicate your feelings with the health care professional, in writing or with the support of someone you wish to accompany you.
You can ask your healthcare professional to stop at any time during your physical examination.
Further information
- National Institute for Health and Care Excellence (NICE) guideline NG88, Heavy Menstrual Bleeding: Assessment and Management
- NHS information on hysteroscopy
- A full list of useful organisations is available on the RCOG website at: https://www.rcog.org.uk/for-the-public/other-sources-of-help
Sources and acknowledgements
This information has been developed by the RCOG Patient Information Committee. It is based on the RCOG Good Practice Paper No. 16, Pain relief and informed decision making for outpatient hysteroscopy procedures, published in February 2023 and on the update of the RCOG Green-top Guideline No. 59, Hysteroscopy, best practice in outpatient, published in August 2024.