This information is for you if you want to know about having a cervical stitch, which is also called cervical cerclage.
You may also find it helpful if you are a partner, relative or friend of someone who is in this situation.
The information here aims to help you better understand your health and your options for treatment and care. Your healthcare team is there to support you in making decisions that are right for you. They can help by discussing your situation with you and answering your
questions.
A glossary of medical terms is available at A-Z of medical terms.
Key points
- You may be offered a cervical stitch if you have a higher chance of giving birth early.
- A cervical stitch may help to keep your cervix closed and may reduce the risk of you having a late miscarriage or a preterm birth.
- A cervical stitch is usually put in between 12 and 24 weeks of pregnancy and then removed at 36–37 weeks, unless you go into labour before this.
A cervical stitch is a procedure in which a stitch is placed around your cervix (the neck of your womb) to try to keep it closed. It is usually done between 11 and 24 weeks of pregnancy, as a planned procedure, although it may be done at later stages in pregnancy and occasionally before pregnancy. It is also called a cervical suture, or cervical cerclage.
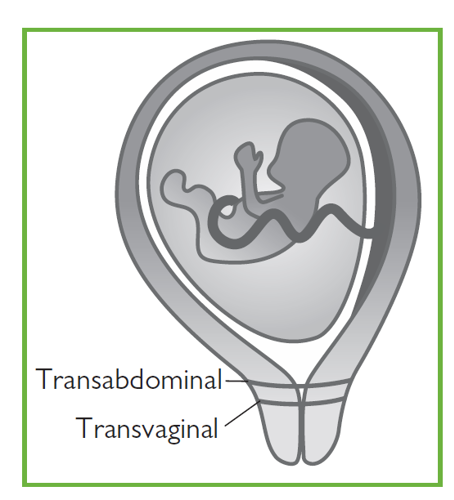
A cervical stitch is more commonly put in vaginally (transvaginal). Less commonly, it is put higher around the cervix by surgery through your abdomen (transabdominal), which can be done as key-hole surgery (laparoscopic). Your healthcare professional will discuss the different types of stitch and which is most suitable for you.
A cervical stitch may be recommended by your health care professional if there is a chance that your cervix may shorten and open too soon. This can lead to an early birth (premature birth) or late miscarriage. A cervical stitch may help to prevent this by keeping your cervix closed.
Babies born early (before 37 completed weeks of pregnancy) can have short- and long-term health problems and may not survive. The chance of health problems is higher the earlier that the baby is born. More information on premature birth can be found at:
https://www.tommys.org/pregnancy-information/premature-birth.
There are many reasons why you may give birth early.
You should be referred to a specialist early in your pregnancy to discuss a plan of care for you if:
- you have had a previous miscarriage after 16 weeks of pregnancy
- you have had a previous birth before 34 weeks of pregnancy
- your waters broke before 34 weeks in a previous pregnancy. See RCOG information When your waters break prematurely
(https://www.rcog.org.uk/en/patients/patient-leaflets/when-your-waters-break-prematurely) - you have had certain types of treatment to your cervix (for example, LLETZ or cone biopsy for treatment of an abnormal smear)
- you have scarring to your endometrium (the lining of your uterus) or your uterus is an unusual shape
- you have had a previous caesarean birth when you were fully dilated (10cm)
- you have needed a cervical stitch in any of your previous pregnancies
Depending on your individual situation, your healthcare team may recommend you to have a planned cervical stitch (a history indicated cervical stitch).
Alternatively you may be offered vaginal ultrasound scans to measure your cervix between 16 and 22 weeks of pregnancy. If the cervix is found to be short (less than 25 mm long), you may be offered:
- a scan-indicated cervical stitch
- a hormonal treatment with progesterone pessaries used daily until 34 weeks
- close monitoring by your healthcare team if you prefer not to have a stitch or the pessaries
Your healthcare professional will discuss the risks and benefits of these options with you depending on your individual circumstances.
Your healthcare professional should discuss the benefits and risks in your individual situation. Sometimes a cervical stitch is not advised because it may carry risks to you and it would not improve the outcome for your baby. This may be if:
- you have any signs of infection
- you are having vaginal bleeding
- you are having contractions
- your waters have already broken.
If you are pregnant with more than one baby, there is no evidence to show that a cervical stitch will prevent you going into labour early and your care will be individualised depending on your situation. See the RCOG patient information Multiple pregnancy: having more than one baby.
Insertion of a cervical stitch takes place in an operating theatre.
You may have a spinal anaesthetic or a general anaesthetic. If
you have a spinal anaesthetic you will stay awake but will be numb
from the waist down. If you have a general anaesthetic you will be
asleep. Your team will discuss these options with you, to allow you
to choose the best option for you.
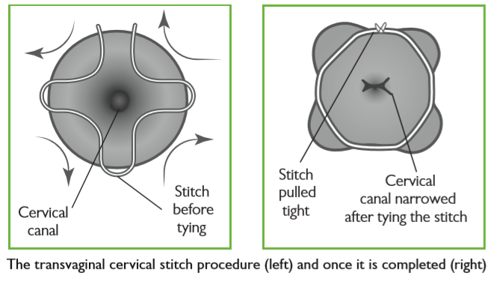
In the operating theatre, your legs will be put in supports and sterile covers will be used to keep the operating area clean. The surgeon will then insert a speculum into your vagina, hold the cervix and put a stitch around it (see the illustration below). The stitch is then tightened and tied, helping to keep the cervix closed. The operation takes less than one hour. You may also have a catheter (tube) inserted into your bladder that will be removed once the anaesthetic has worn off.
You may be offered antibiotics during the operation and you will
be offered medication to ease any discomfort after the surgery.
You are likely to be able to go home the same day or early the following day, although you may be advised to stay in hospital longer depending on your circumstances.
In the image: The transvaginal stitch procedure, viewed looking at the cervix through the speculum. The stitch is first inserted around the opening of the cervix (left); the stitch is pulled tight and completed (right).
This is a less common procedure, also called a “transabdominal cerclage” (TAC), which may be recommended for you if a vaginal cervical stitch has not worked in the past or if it is not possible to insert a vaginal stitch.
It is ideally done before you become pregnant or occasionally in early pregnancy.
It may be done through a cut on your abdomen or via keyhole surgery (laparoscopy). This sort of stitch is not removed and your baby would need to be born by caesarean
Occasionally, you may be offered a cervical stitch as an emergency procedure after your cervix has already opened up, to help prevent you from having a late miscarriage or early preterm birth. This is called an ‘emergency’ stitch and your healthcare team will discuss the risks and benefits of this with you. This type of stitch has higher risks and is less likely to work than other stitches.
The risks of surgery include:
- bleeding
- infection
- injury to your bladder
- injury to your cervix
- your waters breaking early
If your cervix is already too short or too far open it may not be possible to put the stitch in.
Even if the stitch is put in successfully it may not always work and you might still experience a late miscarriage or preterm birth.
If you go into labour with the stitch in place, there is a risk of injury to your cervix during labour. A vaginal cervical stitch should be removed as soon as possible after the start of ![]() labour (more details below) but does not increase your chances of needing a caesarean birth.
labour (more details below) but does not increase your chances of needing a caesarean birth.
After the operation, you may have some vaginal bleeding or brownish discharge for a day or two. You will usually be advised to use a period pad rather than a tampon for the bleeding. You should not feel any significant pain from the stitch. You will usually be advised to rest for the first 2 days.
Once you recover from the operation, you can carry on as normal for the rest of your pregnancy. The plan of care for you and your baby will be discussed with you. Having a stitch in place will not affect your baby’s growth and development. Resting in bed is not routinely recommended. You can have sex when you feel comfortable to do so although occasionally your partner may be able to feel the stitch during sex.
You should contact your healthcare team without delay if you experience any of the following:
- contractions or cramping abdominal pain
- continued or heavy vaginal bleeding
- your waters breaking
- smelly or green vaginal discharge.
Your stitch will be taken out at the hospital. This will normally happen at around 36–37 weeks of pregnancy, unless you go into labour before then, or unless you are having a planned caesarean, in which case the stitch can be taken out at the time of your caesarean.
Removing the stitch is usually a simpler procedure than putting it in. A speculum is inserted into your vagina and the stitch is cut and removed. You will not normally need anaesthetic for removal of the stitch.
It usually takes just a few minutes and you may experience some pain. If the procedure is too painful for you, you can ask your healthcare professional to stop at any time, and your healthcare professional will discuss your pain relief options with you. This may include a
spinal anaesthetic.
You may notice some blood staining or vaginal spotting afterwards. This should settle within 24 hours but you may have a brown discharge for longer. If you have any concerns, you should tell your healthcare professional.
Most women do not go into labour immediately after their stitch is removed.
If you have an abdominal stitch, you will usually be advised to have a planned caesarean birth. The stitch is usually left in for any future pregnancies.
If you go into labour with the cervical stitch still in place, you should contact your maternity unit straight away. It is important to have the stitch removed to prevent damage to your cervix.
If your waters break early but you are not in labour, the stitch will usually be removed because of the increased risk of infection. The timing of this will depend on your individual situation.
If you have had a vaginal stitch in this pregnancy, you may be offered a stitch again in a future pregnancy, or rarely, an abdominal stitch in between pregnancies if a vaginal stitch was not successful for you this time. You should be referred to a specialist clinic to discuss a plan of care for you.
The nature of gynaecological and obstetric care means that physical examinations are often necessary. This may involve an examination of your abdomen or an internal examination of your vagina.
We understand that for some women, including those who have experienced trauma, physical or sexual abuse, such examinations can be very difficult. Your healthcare professionals are there to provide kind and personalised care to you. If you choose not to be examined, they can discuss alternative options with you.
After explaining to you about the physical examination you are being offered, your healthcare professional will seek your consent. You should always be offered a chaperone. This could be a partner, family member, friend, support person or another healthcare professional.
If you feel uncomfortable, anxious, distressed or in pain at any time before, during, or after an examination, please let your healthcare professionals know, as they are there to support you.
If you find this difficult to talk about, you may communicate your feelings in writing or with the support of someone you wish to accompany you.
You can ask your healthcare professional to stop at any time during your physical examination.
Further information
National Institute for Health and Care Excellence (NICE) – Preterm Labour and Birth
If you are asked to make a choice, you may have lots of questions that you want to ask. You may also want to talk over your options with your family or friends. It can help to write a list of the questions you want answered and take it to your appointment.
Ask 3 Questions
To begin with, try to make sure you get the answers to 3 key questions, if you are asked to make a choice about your healthcare:
- What are my options?
- What are the pros and cons of each option for me?
- How do I get support to help me make a decision that is right for me?
*Ask 3 Questions is based on Shepherd et al. Three questions that patients can ask to improve the quality of information physicians give about treatment options: A cross-over trial. Patient Education and Counselling, 2011;84:379-85
Sources and acknowledgements
This information has been developed by the RCOG Patient Information Committee. It is based on the RCOG Green-top Guideline No 75 Cervical Cerclage and on the NICE guideline 25 Preterm Labour and Birth. These guidelines contain a full list of the sources of evidence we have used.